
Anonymous 3m 849 #warondrugs
The views of this article are the perspective of the author and may not be reflective of Confessions of the Professions.
The U.S. government has burned almost enough marijuana plants to get the atmosphere high. Americans have responded by increasing domestic production.
With drug addiction rising, it’s not surprising that more people are seeking information about treatment from Bow Creek rehab center reviews or any other similar resource.
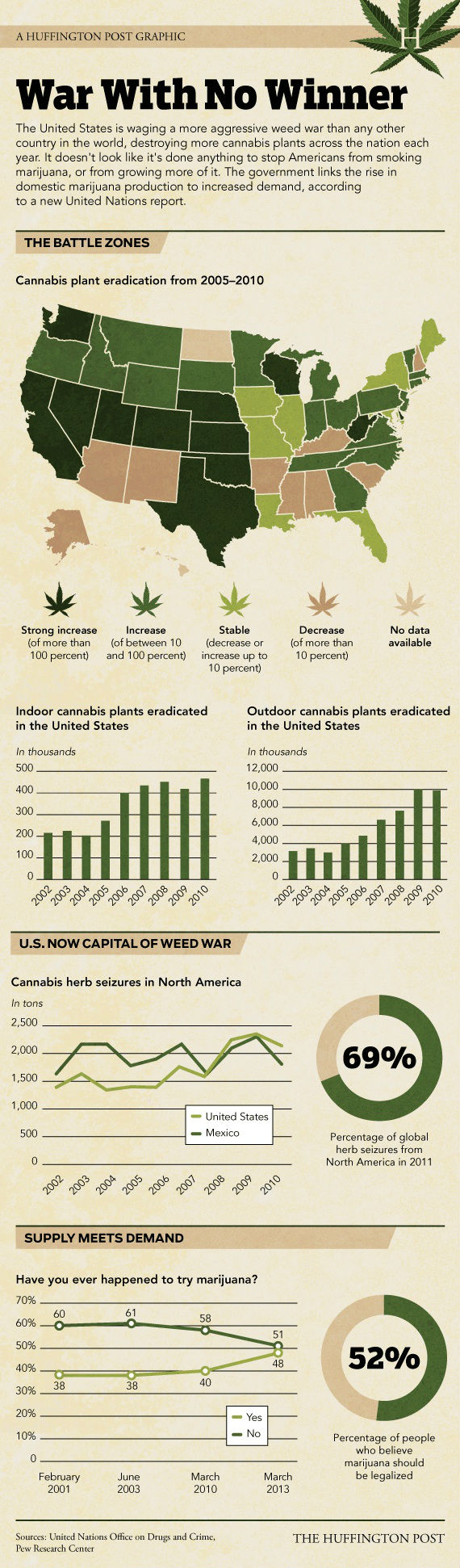
A Huffington Post Graphic: War With No Winner
The United States is waging a more aggressive weed war than any other country in the world, destroying more cannabis plants across the nation each year. It doesn’t look like it’s done anything to stop Americans from smoking marijuana, or growing more of it. The government links the rise in domestic marijuana production to increased demand, according to a new United Nations report.
Click to Open / Right-click for save options
Marijuana in the United States of America
As of February 2013, 18 states of the United States of America, including the District of Columbia, have passed laws allowing marijuana to be used for a variety of medical conditions.
Many of these states have in place, or are developing, programs or provisions to regulate the use of medical marijuana by approved patients, as well as the cultivation, sale and possession of marijuana.b Under the programmes of some states, patients may be assisted by so-called caregivers, who are persons authorized to help patients grow, acquire and use the drug.
In 2012, voters in two states—Colorado and Washington state—also passed initiatives legalizing the sale and recreational use of marijuana by adults, aged 21 years and older.
It is important to note that none of these state marijuana laws changes the fact that producing, selling or possessing marijuana continues to be an offence under United States Federal law. The position of the United States Federal Government is that marijuana should be subjected to the same rigorous clinical trials and scientific scrutiny that are applied to all other new medications.
Medical marijuana laws were passed separately on a state-by-state basis; a wide range of different policies regulating marijuana use exist. Nevada, for example, allows the possession of 1 ounce (28 grams) of usable marijuana, three mature and four immature plants.
Oregon permits patients to possess up to 24 ounces (672 grams) of usable marijuana and six mature plants. Though most states that have decriminalized medical marijuana have also provided legal protections for its users, the majority of these laws have not established mechanisms for dispensing the drug or for regulating its quality and safety.
The definitions of what qualifies patients for medical marijuana can vary greatly among these states. New Mexico, for instance, permits the use of medical marijuana only for a limited set of conditions (including cancer, glaucoma, HIV/AIDS, epilepsy, multiple sclerosis, spinal cord damage and terminal illness). California, on the other hand, has an extensive list that includes general ailments such as migraines, severe or chronic pain and “any other illness for which marijuana provides relief.”
Data on numbers of and trends among medical marijuana patients are limited by the absence of a standard method of
collecting and disseminating data. Many states have a mandatory registration system of patients; in California, the most
populous United States state, registration is voluntary. Only some states, such as Colorado, provide detailed statistics
online.
A recent study examined a number of state medical marijuana registries as of June 2011 (in states with mandatory
registration only) and highlighted some key information about those enrolled in medical marijuana programmes. The
study concluded that the majority of persons registered appeared to be young, male and registered for chronic pain. There
was a significant difference between states in the proportion of the adult population registered for medical marijuana,
ranging from 4.1 per cent (Montana) to 0.07 per cent (Vermont). Possible explanations given for these differences were
differences in disease burden, social acceptance of marijuana and ease of marijuana registration and acquisition. The
study was limited by a lack of or limited data from several states.
There is an ongoing discussion on the impact of medical marijuana laws on overall levels of marijuana use and on risk
perception of consumption. Several articles on that topic are listed below.
Further reading
Sunil K. Aggarwal and others, “Medicinal use of cannabis in the United States: historical perspectives, current trends,
and future directions”, Journal of Opioid Management, vol. 5, No. 3 (2009), pp. 153-168.
Magdalena Cerdá and others, “Medical marijuana laws in 50 states: investigating the relationship between state legalization of medical marijuana and marijuana use, abuse and dependence”, Drug and Alcohol Dependence, vol. 120, No. 1
(2012), pp. 22-27.
Dennis M. Gorman and Charles Huber, Jr., “Do medical cannabis laws encourage cannabis use?”, International Journal
of Drug Policy, vol. 18, No. 3 (2007), pp. 160-167.
Sam Harper, Erin C. Strumpf and Jay S. Kaufman, “Do medical marijuana laws increase marijuana use? Replication
study and extension”, Annals of Epidemiology, vol. 22, No. 3 (2012), pp. 207-212.
Shereen Khatapoush and Denise Hallfors, “‘Sending the wrong message’: did medical marijuana legalization in California change attitudes about and use of marijuana?”, Journal of Drug Issues, vol. 34, No. 4 (2004), pp. 751-770.
Robin Room and others, Cannabis Policy: Moving Beyond Stalemate (Oxford, Oxford University Press, 2010).
Source: http://www.unodc.org/doc/wdr/Chp1_C.pdf
Infographic by Jan Diehm for The Huffington Post.
(
![Practice Makes Perfect [Infographic]](https://cdn.statically.io/img/cdn.confessionsoftheprofessions.com/media/2018/08/practice-makes-perfect-1.jpg?quality=100&f=auto "Practice Makes Perfect [Infographic]")
![Should I Go to Grad School? [Infographic]](https://cdn.statically.io/img/cdn.confessionsoftheprofessions.com/media/2018/08/grad-school.jpg?quality=100&f=auto "Should I Go to Grad School? [Infographic]")
![What Kind of Smart Are You? [Infographic]](https://cdn.statically.io/img/cdn.confessionsoftheprofessions.com/media/2018/08/brain-intelligence.jpg?quality=100&f=auto "What Kind of Smart Are You? [Infographic]")
![How To Love Your Job [Infographic]](https://cdn.statically.io/img/cdn.confessionsoftheprofessions.com/media/2018/08/love-my-job-mug.jpg?quality=100&f=auto "How To Love Your Job [Infographic]")
![Behind Personality Tests [Infographic]](https://cdn.statically.io/img/cdn.confessionsoftheprofessions.com/media/2018/08/personality-awareness.jpg?quality=100&f=auto "Behind Personality Tests [Infographic]")
![Tips To Market Yourself as a Web Designer [Infographic]](https://cdn.confessionsoftheprofessions.com/infographics/market-self-infographic.jpg "Tips To Market Yourself as a Web Designer [Infographic]")